Picture walking into a specialist clinic today. You don’t carry a battered file stuffed with old prescriptions, faded thermal-printed ultrasound reports, or CD-ROMs containing your MRI scans. Instead, you scan a QR code at the reception desk using your Ayushman Bharat Health Account (ABHA) application. Within seconds, the attending physician pulls up your entire medical history on their screen. It feels like magic, but behind that frictionless moment is a fiercely regulated, highly complex digital infrastructure. In today’s healthcare landscape, secure data sharing isn’t just a neat technical trick; it is governed by the heavy hand of the Digital Personal Data Protection (DPDP) Act of 2023.
If you manage a hospital, build health-tech software, or run a diagnostic lab, you already know the ground shifted beneath your feet. The Ayushman Bharat Digital Mission (ABDM) opened the floodgates for interoperability and data sharing, allowing medical records to flow freely across the country. But that freedom comes with absolute liability. You can no longer treat patient information as an institutional asset. You are merely its custodian. Let’s strip away the heavy legalese and look at what it actually takes to legally route a patient’s medical history across India’s digital health grid without triggering catastrophic fines.
The Collision of Convenience and Absolute Privacy
To understand the current ecosystem, you have to look at the two massive forces shaping it. On one side, you have the National Health Authority (NHA) pushing the ABDM framework. Their goal is radical interoperability and seamless data sharing. They want unique IDs (ABHA), verified registries for doctors and facilities, and a unified interface where a clinic in rural Kerala can instantly pull a discharge summary from a mega-hospital in Mumbai.
On the other side, you have the DPDP Act. This legislation treats personal information—especially health information—like radioactive material. It demands that every single byte of information transferred between entities happens with undeniable, granular, and perfectly logged permission.
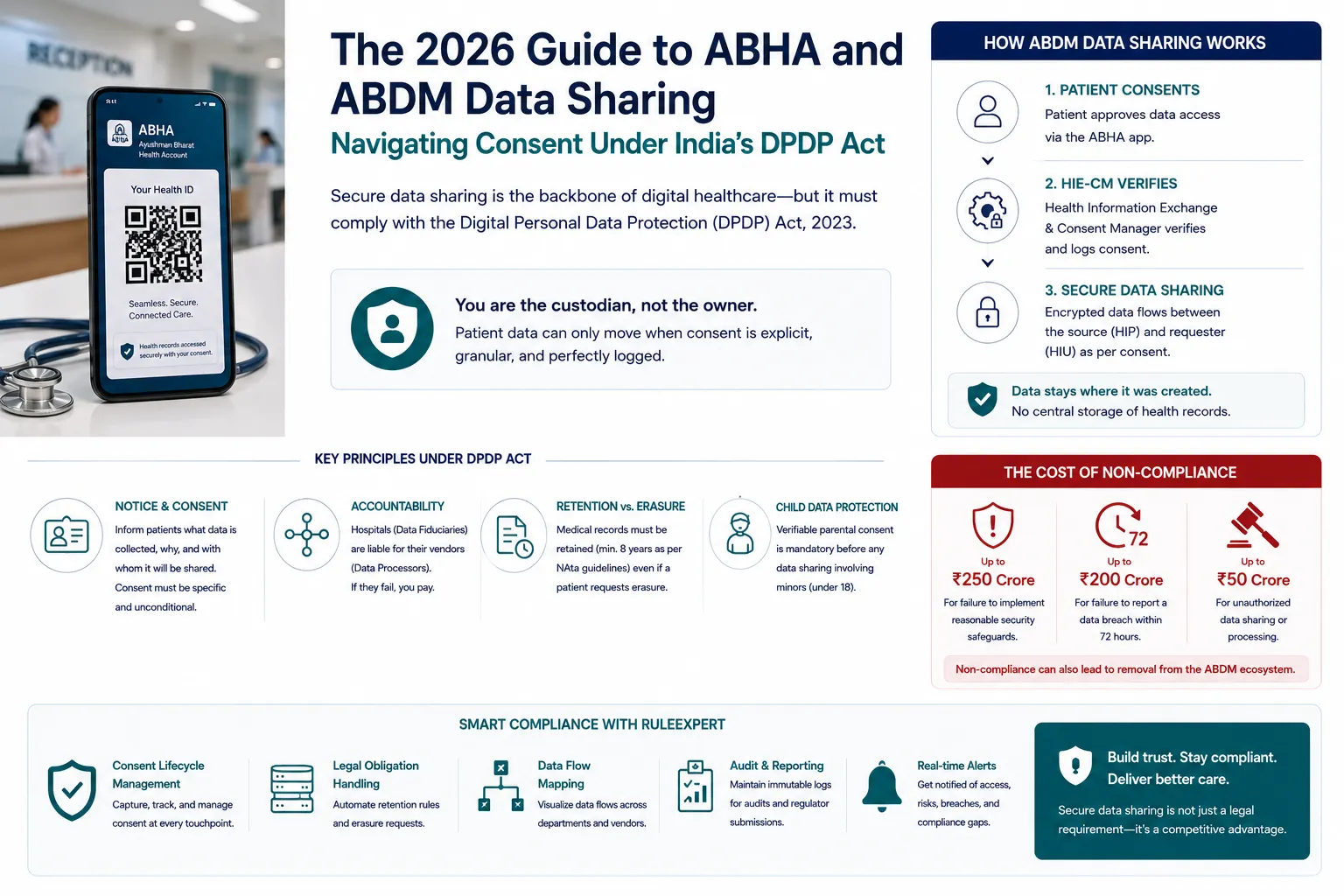
So, how do these two forces coexist? They meet at the consent architecture. Medical data sharing under the ABDM is strictly federated. There is no massive, centralized government server hoarding everyone’s health records. The data stays exactly where it was created—at the local hospital’s server or their chosen cloud provider. When a patient uses their ABHA app to approve a transfer, the Health Information Exchange and Consent Manager (HIE-CM) acts as an invisible traffic cop. It verifies the patient’s approval and then temporarily unlocks the encrypted tunnel between the hospital holding the data (the Health Information Provider, or HIP) and the doctor requesting it (the Health Information User, or HIU).
Rewriting the Operational Playbook for Hospitals
Before these regulations matured, healthcare compliance was mostly about securing physical files and making sure the IT guy installed a firewall. A patient signed a dense, ten-page admission form that included a vague clause about “using information for treatment and operations.” That bundled consent is now legally useless.
Under the DPDP Act, data sharing demands a notice-based, explicit approach. You have to tell the patient exactly what you are doing, why you need to do it, and who else is going to see their information. And you have to do this in plain language, not impenetrable medical jargon.
Let’s look at a routine surgery. A hospital collects a patient’s vitals, runs blood panels through a third-party diagnostic lab, sends imaging to an outsourced radiology center, and coordinates with an insurance Third-Party Administrator (TPA) for cashless approval. Every single one of these hops involves sensitive data sharing.
The Hospital
- Data Fiduciary — they determine the purpose of the processing.
Labs, Cloud Hosts, TPAs
- Data Processors — they act on the hospital’s instructions.
If that radiology center suffers a data breach, or if the TPA uses the patient’s medical history to quietly build a risk profile for future marketing through unauthorized data sharing, the hospital is on the hook. The DPDP Act doesn’t care if your vendor messed up. The fiduciary holds the ultimate liability. This is why mapping your digital supply chain has become the most critical administrative task for modern healthcare administrators.
The Tightrope Walk: Retention vs. Erasure
Here is where things get genuinely tricky for hospital compliance officers. The DPDP Act grants patients the explicit right to erasure. If a patient revokes their consent, they can demand that you scrub their digital footprint from your systems.
But healthcare doesn’t exist in a vacuum. The NHA’s Health Data Management Policy (HDMP) and various clinical establishment rules mandate that hospitals must retain patient health records for a minimum of eight years after the last consultation. These retention requirements continue to apply even when patients place restrictions on data sharing. You cannot simply delete a surgical record just because the patient asked you to; doing so would violate medical governance laws and open doctors up to severe malpractice liabilities.
Managing this statutory conflict manually is a nightmare. A front-desk employee cannot be expected to evaluate the legal hierarchy of a patient’s deletion request against NHA retention guidelines. This operational friction is driving the rapid adoption of compliance middleware.
- Patient Requests Erasure
↓ - RuleExpert audits the file
↓ - Recognizes clinical retention mandate (NHA, 8-year rule)
↓ - Isolates record from routine data sharing environments
↓ - Generates legally sound denial notice, citing the NHA guideline
Systems like RuleExpert have become essential invisible engines inside hospital networks. Instead of relying on human judgment for every request, automation platforms implement a “Legal Obligation Override.” It bridges the gap between patient rights and medical reality without requiring a lawyer in the room.
The Pediatric Dilemma and Age-Gating
If managing adult records is complex, pediatric data is a veritable minefield. Section 9 of the DPDP Act places intense restrictions on processing children’s data. You cannot simply rely on a parent signing a physical form in the pediatric ward anymore.
Whenever a hospital engages in data sharing involving a minor’s health records, they must execute verifiable parental consent. This means integrating age-gating mechanisms directly into the hospital’s digital intake software. It involves verifying the identity of the guardian, logging their relationship to the child, and maintaining that consent trail until the child turns eighteen. At that point, the system must technically pause processing until the new adult ratifies the consent themselves. Trying to track this lifecycle on Excel spreadsheets is a guaranteed path to a regulatory audit.
The True Cost of Getting It Wrong
Why is the industry suddenly taking this so seriously? Because the financial penalties have moved from slap-on-the-wrist territory to extinction-level events.
- ₹250 Crore: Failure to implement reasonable security safeguards, resulting in a breach of patient health records
- ₹200 Crore: Failing to notify the Board and affected patients about a breach
- ₹50 Crore: Unauthorized data sharing — e.g. slipping patient analytics to a research firm without specific consent
Beyond the financial ruin, non-compliance means getting cut off from the ABDM registry. A hospital that loses its HIP/HIU status essentially disappears from the national digital health grid. In an era where patients expect seamless digital experiences, losing interoperability is a death sentence for a healthcare business.
Looking Ahead: Building for Trust
We are moving past the phase where compliance was just a box to check. The intersection of the DPDP Act and the Ayushman Bharat Digital Mission has fundamentally altered the relationship between a patient and their doctor. Health information is now recognized as a deeply personal extension of the individual, making consent-driven data sharing a central pillar of modern healthcare governance.
For clinics, diagnostic centers, and health-tech innovators, this isn’t just about avoiding catastrophic fines. It’s about competitive advantage. Patients are becoming increasingly aware of their digital rights. A healthcare provider that can transparently demonstrate how tightly they guard medical histories will earn a profound level of trust.
Embracing rigorous data sharing protocols, deploying smart automation tools to handle the heavy lifting, and respecting the boundaries of patient consent is how the next generation of healthcare leaders will separate themselves from the pack.
Frequently Asked Questions
1. What exactly constitutes health data sharing under the DPDP Act?
It covers any digital transfer of a patient’s medical information. This includes everything from a doctor pulling up an ABHA-linked health record, to a hospital sending blood samples to a third-party pathology lab, to sharing discharge summaries with an insurance company for claims processing. If digital health information moves from one entity to another, it falls under the regulatory umbrella.
2. Does the DPDP Act override or replace the NHA Health Data Management Policy?
No, they work together. The DPDP Act provides the overarching legal framework for all personal data in India, defining penalties, rights, and broad obligations. The NHA’s HDMP provides the specific, domain-level guidelines for how those principles apply specifically within the ABDM ecosystem. Where conflicts arise—like data retention versus the right to erase—specific clinical laws generally provide exceptions to the DPDP’s deletion mandates.
3. How does the ABHA application actually manage patient consent?
The system relies on the Health Information Exchange and Consent Manager (HIE-CM). When a doctor requests your records, a notification pings your ABHA app. You can review exactly what data is being requested, by whom, and for how long. You then generate a “Consent Artefact” (a secure, logged digital token). Only with this token will the system allow the encrypted data sharing to proceed.
4. What is the penalty for unauthorized data sharing under the new framework?
The financial consequences are severe. Processing patient data without valid, granular consent can result in fines up to ₹50 crore. If poor security practices lead to a data breach, the penalties can soar up to ₹250 crore per incident, alongside immense reputational damage.
5. How do hospitals handle the conflict between keeping records and a patient’s right to erase them?
This is where technology plays a huge role. While the DPDP Act allows patients to request the erasure of their data, hospitals are legally bound by NHA guidelines to keep clinical records for at least eight years. Hospitals use compliance software to log the patient’s request but issue a legal denial based on statutory retention requirements, securely archiving the data so it isn’t used for anything other than legal compliance.
6. Can medical data be shared with insurance companies without explicit patient approval?
Absolutely not. Bundled consent is dead. A patient must provide specific, separate consent for their medical data to be shared with a Third-Party Administrator (TPA) or insurance provider. This ensures that a hospital cannot quietly pass clinical histories to insurers without the patient knowing exactly what is being sent.
7. How does the consent architecture work for minors or pediatric patients?
Under Section 9 of the DPDP Act, anyone under 18 cannot legally give consent for their own data processing. Hospitals must implement verifiable age-gating and obtain explicit consent from a parent or legal guardian before any data sharing occurs regarding a minor’s health records.
8. Are healthcare providers required by law to use third-party compliance tools like RuleExpert?
The law does not mandate the use of any specific commercial software brand. However, the law does mandate strict audit trails, granular consent logs, breach notifications, and complex data lifecycle management. Handling these requirements manually using paper or basic spreadsheets is functionally impossible at the scale of a modern hospital, making automated compliance platforms a practical necessity, even if not explicitly named in the legislation.