Walk into any major Indian hospital today, and the real heartbeat isn’t just blipping away on the patient monitors in the ICU. It’s humming inside the server rooms. To deliver seamless care, coordinate instantly across departments, and process complex insurance claims without skipping a beat, nearly every modern medical facility relies heavily on an electronic health record system. But as the healthcare sector aggressively expands its digital footprint, that exact same system has suddenly morphed into your biggest legal vulnerability.
On November 14, 2025, the Ministry of Electronics and Information Technology (MeitY) finalized and officially notified the DPDP Rules 2025, breathing full operational life into the Digital Personal Data Protection (DPDP) Act of 2023. The grace periods are largely mapping out, and the regulatory leniency window is slamming shut. For hospital administrators, IT directors, and chief medical officers, the most pressing board-level question isn’t just about general baseline privacy anymore. The multi-crore question keeping executives awake is whether your facility’s data operations—including the management of every Electronic Health Record System—officially classify you as a Significant Data Fiduciary (SDF).
If you catch the SDF label, standard compliance goes completely out the window. You enter a brutal tier of hyper-regulation. So, where does your hospital actually stand? Let’s pull apart the official, confirmed mandates of the DPDP Act and see what happens when the government puts your clinical data infrastructure and Electronic Health Record System under the microscope.
The Reality of Section 10: What Exactly is an SDF?
Before we dive into the clinical side of things, we need to strip away the jargon and look at what the law actually says. Under Section 10(1) of the DPDP Act 2023, the Central Government holds the absolute authority to designate certain organizations as a Significant Data Fiduciary, including hospitals and healthcare providers that process large volumes of patient information through an electronic health record system.
They don’t just hand this title out arbitrarily. The classification is built on a very specific, unforgiving set of parameters:
- The volume and sensitivity of the personal data processed.
- The risk of harm to the rights of the Data Principal (your patients).
- The potential impact on the sovereignty and integrity of India.
- The risk to electoral democracy.
- The security of the State and public order.
While a neighborhood clinic treating twenty people a day might easily remain a standard Data Fiduciary, a multi-specialty hospital chain is playing an entirely different game. When you plug thousands of new patient histories into an electronic health record system every single week, you slam into the “volume and sensitivity” threshold almost instantly.
Why Healthcare is Sitting Dead Center in the Regulatory Crosshairs
Let’s be brutally honest—a hospital doesn’t collect basic, harmless data. You aren’t a retail app asking for a zip code and an email address. The data flowing through your fiber optics is the most intimate, sensitive, and potentially damaging information a human being can generate.
Every time a specialist updates a chart, your electronic health record system digests biometric markers, genetic information, mental health diagnoses, substance abuse histories, and chronic illness records. Add in the financial data from the billing departments and the KYC documents required for insurance, and you have built a massive, centralized goldmine for cybercriminals.
The government is acutely aware of this. Under the newly notified framework, the “risk to the rights of the Data Principal” serves as a massive trigger for SDF classification. If an e-commerce site gets hacked, someone might have to deal with fraudulent credit card charges. If a hospital’s electronic health record system gets breached, patients face severe psychological distress, targeted workplace discrimination, social stigma, and unquantifiable personal harm.
Because the stakes of a medical data leak are catastrophic, the Central Government views large-scale healthcare providers as prime, obvious candidates for the SDF designation.
The “Big Three” Triggers That Could Tip Your Hospital into SDF Territory
You might be thinking, “We are a mid-sized regional hospital, not a national corporate chain. We’ll fly under the radar.” Don’t bet on it. The DPDP Rules 2025 focus heavily on the nature and velocity of the data, not just the brand name printed on the building. Here is exactly what the regulatory bodies are weighing, especially when that data is being continuously collected, updated, and shared through an electronic health record system:
1. The Sheer Velocity of Integrated Data
It’s not just about how many physical beds you have. It’s about outpatient numbers, telemedicine application consultations, and diagnostic lab integrations. If your electronic health record system is constantly pulling API data from third-party pathology labs, pharmacy chains, and patient health wearables, your digital data volume is exponentially higher than your actual foot traffic.
2. The Permanence of Medical Records
Unlike a quick retail transaction that is processed and forgotten, medical records linger. In many cases, they are legally kept for the lifetime of the patient. Storing massive, compounding archives of historical health data naturally increases your risk profile year over year, making you look much larger to auditors.
3. Algorithmic and AI Processing
Are you using AI-driven diagnostic screening tools? Are you running predictive analytics to anticipate patient ICU readmissions? Under Rule 13 of the new DPDP framework, utilizing complex algorithmic software to modify, share, or analyze personal data drastically increases the likelihood of government scrutiny and SDF tagging.
You Got Classified as an SDF. What Happens Next?
Let’s say the notification arrives on your desk. The Central Government has officially classified your hospital network as a Significant Data Fiduciary. What actually changes on Monday morning?
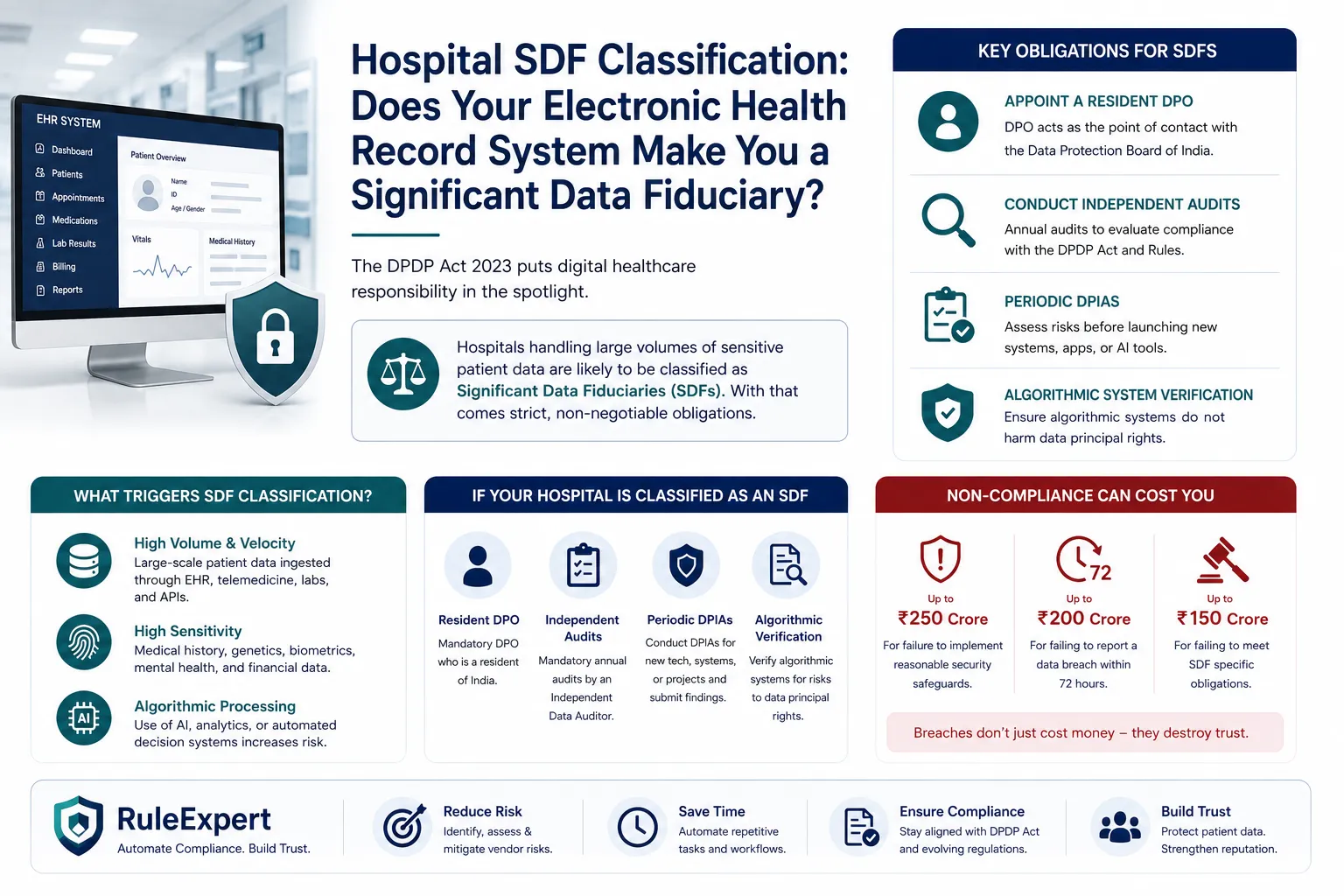
In short: everything. Standard fiduciaries have to collect consent and quietly secure data. SDFs have to actively prove they are doing it, constantly and loudly, to the government. Here are your official, non-negotiable legal obligations:
Appointing a Resident Data Protection Officer (DPO)
You can no longer just hand this job to your overworked IT lead as a secondary task. You must appoint a dedicated Data Protection Officer who legally resides in India. This individual becomes the lightning rod for your hospital. They act as the direct point of contact for the Data Protection Board of India, and the law dictates they must report directly to your hospital’s Board of Directors or governing body while overseeing compliance across critical systems such as the Electronic Health Record System.
Mandatory Independent Data Audits
Say goodbye to comfortable internal self-assessments. SDFs are legally required to appoint an Independent Data Auditor. This third-party entity will come in, rip open the backend of your electronic health record system, and evaluate every single data flow, consent log, and security protocol to ensure it aligns perfectly with the DPDP Act 2023.
Periodic Data Protection Impact Assessments (DPIA)
Before you roll out a new telemedicine feature, or upgrade the core modules of your electronic health record system, you must conduct a DPIA. This is a formal, heavily documented process that assesses the core necessity of the data collection, identifies potential privacy risks to the patients, and outlines exactly how you plan to mitigate those risks. You have to submit the significant findings of these assessments directly to the Data Protection Board.
Algorithmic Verification
As per the newly clarified Rule 13, if your hospital uses algorithmic software to process, host, or display data—including applications integrated with your Electronic Health Record System—you must actively verify that this software doesn’t pose a risk to your patients’ rights. You can no longer blindly trust third-party software vendors; the legal burden of algorithmic fairness and safety now rests entirely on the hospital’s shoulders.
The ₹250 Crore Reality Check
We have to talk about the penalties. The Data Protection Board of India wasn’t established to write polite warning letters or give slaps on the wrist. The DPDP Act has vicious teeth, and the financial repercussions for a healthcare provider can be completely devastating.
- ₹250 CroreFailure to maintain reasonable security safeguards — lacking proper encryption, role-based access controls, or data masking when a breach occurs
- ₹200 CroreFailure to report a breach to the Board and affected patients within the mandatory 72-hour window
- ₹150 CroreFailure to meet SDF obligations — skipping the independent audit or failing to appoint a proper DPO
This isn’t just a quirky IT problem anymore. It’s an existential business threat. A single major compliance failure could wipe out a hospital’s entire operating budget for the fiscal year.
Rebuilding the Tech Stack: Closing the Compliance Gap
How does a hospital actually survive this tectonic regulatory shift? You absolutely cannot manage DPDP compliance with chaotic spreadsheets and dusty paper consent forms stacked at the reception desk. The moment an angry patient demands their “Right to Erasure” (Section 12), you need to be able to locate and delete their non-essential data across every server, backup drive, and department instantly.
Your electronic health record system must evolve into a fortress of verifiable consent. This means integrating automated compliance workflows directly into the physical patient admission process. When a patient signs in, their consent must be itemized, specific, and unconditional. If they withdraw consent via a patient portal app later that week, your backend systems must automatically flag and restrict their data from further processing.
This is exactly where advanced automation becomes non-negotiable. Smart hospitals are increasingly bolting dedicated compliance software onto their existing tech stacks and Electronic Health Record System environments to handle the heavy lifting. Solutions like RuleExpert allow healthcare providers to seamlessly map complex data flows, automate those tedious Data Protection Impact Assessments, and maintain the immutable audit logs that the Independent Data Auditor will inevitably demand. By automating the friction out of compliance, medical staff can get back to focusing on saving lives rather than stressing over data governance.
The Bottom Line
The era of “move fast and break things” in digital healthcare is officially dead. With the DPDP Rules 2025 now fully operational, the Indian government has made it abundantly, legally clear that patient data stored, processed, and exchanged through every Electronic Health Record System is not a commodity—it is a fiercely protected right.
Whether your hospital network is officially notified as a Significant Data Fiduciary tomorrow morning, or you are simply preparing your infrastructure for future scale, the mandate remains identical. You must secure your digital perimeter. Evaluate your electronic health record system, appoint the right experts, and automate your compliance before an audit—or worse, a catastrophic breach—forces your hand.
Nitin Ray is a Compliance Manager at RuleExpert with expertise in DPDP compliance, data privacy, consent management, and governance. He helps organizations implement practical compliance frameworks and automation strategies to meet the requirements of India’s Digital Personal Data Protection Act, 2023.
Frequently Asked Questions (FAQs)
1. What exactly triggers Significant Data Fiduciary (SDF) status for a hospital under the DPDP Act?
Under Section 10 of the DPDP Act, the Central Government designates SDFs based on several factors, primarily the volume and sensitivity of the personal data processed, and the inherent risk to the rights of the Data Principals (patients). Because hospitals handle highly sensitive medical and financial data at a massive scale, large healthcare networks are at a very high risk of being officially notified as SDFs.
2. Does our electronic health record system need to be hosted exclusively in India?
The DPDP Act allows for cross-border data transfers by default, except to countries explicitly blacklisted by the government. However, under the Rules 2025, an SDF faces much tighter scrutiny. A government-appointed committee can mandate that certain specified personal data processed by an SDF cannot be transferred outside the territory of India at all.
3. What is the exact penalty if a hospital ignores its SDF obligations?
If an entity notified as an SDF fails to fulfill its specific, enhanced obligations—such as conducting Data Protection Impact Assessments or appointing an Independent Data Auditor—they can face brutal financial penalties reaching up to ₹150 Crore under the official schedule of the DPDP Act.
4. Who is eligible to act as a Data Protection Officer (DPO) for a hospital?
If classified as an SDF, a hospital must appoint a Data Protection Officer who is a legal resident of India. This individual cannot just be an entry-level IT staffer; they must be a qualified individual authorized to represent the hospital, act as the primary point of contact for the Data Protection Board, and answer directly to the hospital’s Board of Directors.
5. What is a Data Protection Impact Assessment (DPIA) in a healthcare context?
A DPIA is a mandatory, rigorous process for SDFs designed to identify and minimize the data protection risks of any new project. For a hospital, this means before implementing a new electronic health record system, launching a patient-facing app, or using AI for diagnostics, you must formally assess the risks to patient privacy, detail mitigation strategies, and submit those findings to the Board.
6. Do hospitals actually need to report minor or seemingly harmless data breaches?
Yes, without exception. Under Rule 7 of the DPDP Rules 2025, Data Fiduciaries must notify the Data Protection Board and the affected individuals of a personal data breach within 72 hours of becoming aware of it. There is currently no “harm threshold” exemption written into the law; all breaches compromising personal data must be reported.
7. How does the DPDP Act handle the medical records of children?
Section 9 strictly mandates that before processing the personal data of a minor (under 18 years of age), the hospital must obtain verifiable parental or guardian consent. Furthermore, hospitals are strictly prohibited from tracking, behaviorally monitoring, or directing any form of targeted advertising at children.
8. Are third-party diagnostic labs considered Data Fiduciaries or Data Processors?
It entirely depends on their operational role. If the lab independently determines the purpose and means of processing the patient’s data, they are a Data Fiduciary in their own right. If they strictly process data only on the explicit, documented instructions of the hospital, they act as a Data Processor. However, the hospital (the primary Fiduciary) remains legally responsible for ensuring that the Processor complies with the DPDP Act’s strict security standards.
2 Comments
Comments are closed.